

 Epiphyseal injury involving the ulnar epiphysis at the wrist and fracture radius are not common and presents a therapeutic challenge. This case of a young adolescent male who presented with such an injury after a fall. he had a Salter-Harris Type 1 epiphyseal injury involving the distal end of the ulna and fracture radius. he was treated with gentle manipulation under anesthesia and stabilization with K-wires. I recommend early reduction and gentle manipulation for these injuries.
Epiphyseal injury involving the ulnar epiphysis at the wrist and fracture radius are not common and presents a therapeutic challenge. This case of a young adolescent male who presented with such an injury after a fall. he had a Salter-Harris Type 1 epiphyseal injury involving the distal end of the ulna and fracture radius. he was treated with gentle manipulation under anesthesia and stabilization with K-wires. I recommend early reduction and gentle manipulation for these injuries. Complications involve growth disruption, possible length discrepancy between the radius and ulna, deformity, injury to the triangular fibro cartilagenous complex, median neuropathy and ulnar shortening seen in 55% of patients. However, most patients were asymptomatic and only a few patients need surgery. Walsh et al. reported that 4% of all wrist injuries presented with Galeazzi injuries. The anatomic reduction of the ulnar injury is paramount for the integrity of the distal radioulnar joint. Most patients with physeal injuries around the wrist have some degree of growth disruption with consequent deformity, but remain clinically asymptomatic.
The injuries to the growth plate were originally classified by Salter and Harris in 1963.
- Type I – transverse fracture through the physis, 6% incidence.
- Type II – A fracture above the physis 75% incidence,
- Type III – A fracture below the physics 8% incidence
- Type IV – A fracture through all three elements of the bone, the physics, above and below it, 10% incidence
- Type V – A compression fracture of the physics, 1% incidence
Case presentation
A 10 year old right-hand dominant boy, presented to the emergency unit with a recent history of fall on outstretched hand. He complained of severe pain, moderate swelling, limitations of movement and a deformity of his wrist.
There were no injuries to the neurological or vascular structures. There were no associated external injuries. Standard antero posterior and lateral X rays of the wrist were performed. The X-rays showed physeal injuries to the distal ulna as well as the fracture of radius, Figure 1. Near total displacement of ulnar epiphysis in the ulnar and dorsal directions was noted. It was initially graded as Type 1 Salter-Harris injury.

{kind=link}
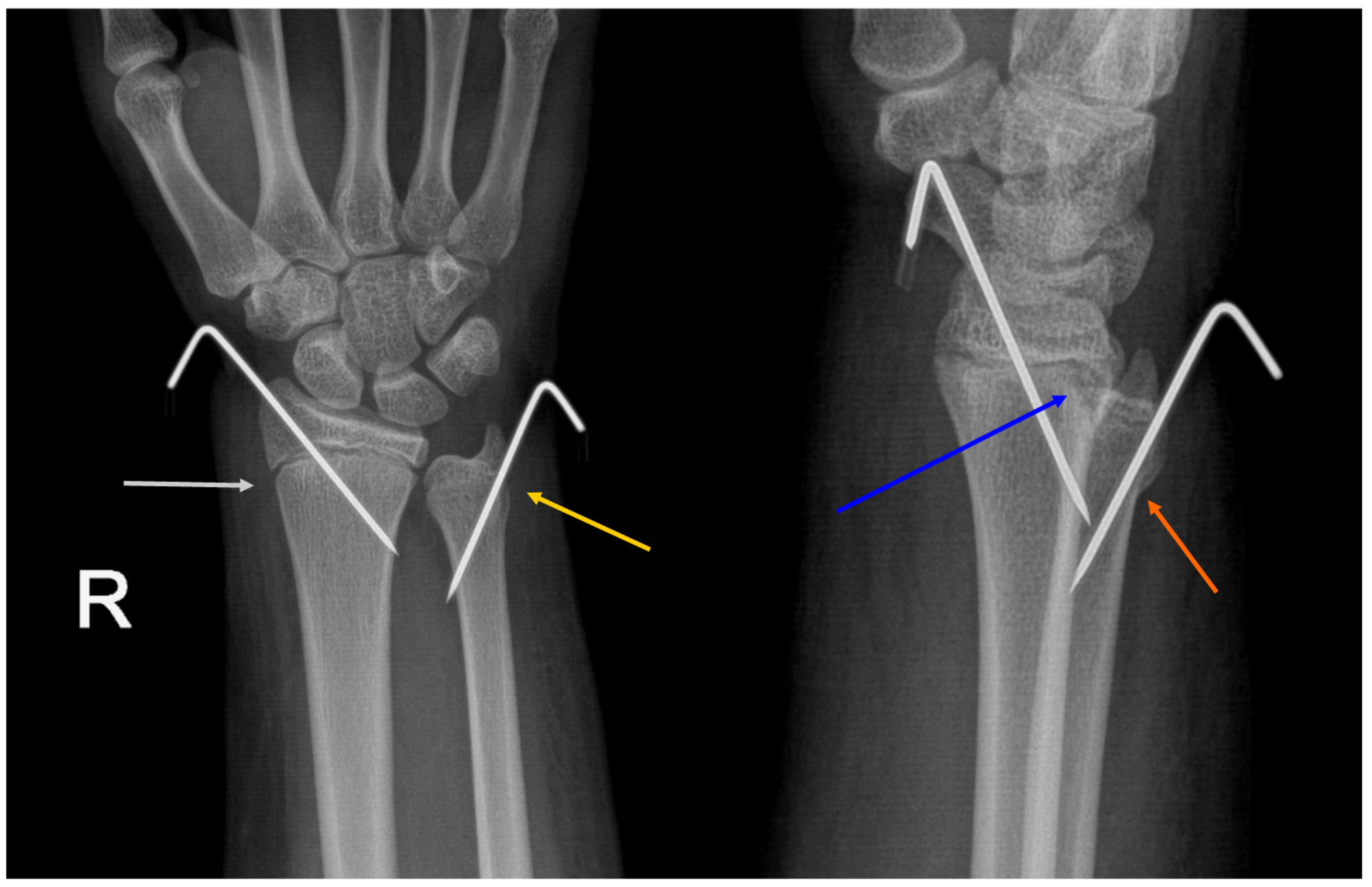
The patient was taken up for closed reduction on the same day. Under anesthesia, the epiphyseal fracture was reduced with longitudinal traction. Minimal and gentle manipulation was only needed to reduce both the radial and ulnar injuries. C-arm images were done. The fluoroscopic images showed instability in the ulnar fracture. Both the fractures were stabilized with smooth 1.2 mm K-wires. The arm was casted with above elbow plaster cast. Post-op X rays were done, figure 2.
K wires were removed after one month and I did another cast for 10 days after checking elbow range of movement, figure 3. Finally cast was removed
